
This website contains information intended solely for healthcare professionals. It is not meant for patients or the general public and should never replace professional medical advice, diagnosis, or treatment. Patients should not rely on this content for decisions about their health or medical care. If you are a patient and have questions about a CooperSurgical Genomics test or its implications, please contact your healthcare provider. Your provider can explain the benefits, risks, and limitations of the test and help determine whether it is appropriate for you.
PGT-A with Select Syndrome ScreenSM detects specific additional genetic abnormalities before embryo transfer.1 Delivering deeper insights without adding complexity to your workflow.

Select Syndrome ScreenSM Helps to change that.
Powered by CooperSurgical’s exclusive PTA technology, this test analyzes smaller sections of DNA to detect 10 specific impactful microdeletion and microduplication syndromes in PGT-tested embryos.4
What are microdeletions and microduplications?
Understanding the genetic changes that may impact embryo viability or health and development after birth.
- Microdeletions: Small segments of missing chromosomes that may lead to developmental, cognitive, or medical challenges.
- Microduplications: Extra copies of chromosome segments that may result in variable and sometimes unpredictable symptoms.
Syndromes detectable with Select Syndrome ScreenSM
Select Syndrome ScreenSM includes 10 impactful genetic disorders that may significantly impact a child’s health or development.4,6
Below is an overview of the 10 syndromes.1
| Syndrome | Description | Genomic region | Estimated occurrence |
|---|---|---|---|
| 22q11.2 deletion syndrome (DiGeorge/Velo-Cardio-Facial syndrome) | Affects heart, immune system, and development | 22q11.2 | 1 in 2,000 births |
| 1p36 deletion syndrome | Causes intellectual disability, seizures, and heart defects | 1p36 | 1 in 5,000 births |
| Wolf-Hirschhorn syndrome | Characterized by distinct facial features, seizures, and growth delays | 4p16.3 | 1 in 20,000 births |
| Cri-du-chat syndrome | Causes high-pitched cry in infancy, cognitive impairment | 5p15 | 1 in 20,000 births |
| Jacobsen syndrome | Leads to intellectual disability, heart defects, and bleeding disorders | 11q23-qter | 1 in 100,000 births |
| 2q33.1 deletion syndrome | Associated with speech delays, facial dysmorphisms, and feeding difficulties | 2q33.1 | Rarer, exact prevalence unknown |
| Potocki-Lupski syndrome | A duplication syndrome linked to autism, hypotonia, and cardiac issues | 17p11.2 | 1 in 25,000 births |
| Smith-Magenis syndrome | Distinctive facial and physical features, mild-to-moderate intellectual disability, sleep and behavioral issues. Also variable vision, hearing, heart, and kidney issues. | 17p11.2 | 1 in 15,000 to 1 in 25,000 births |
| Langer-Giedion syndrome | Causes skeletal abnormalities, intellectual disability, and distinctive facial features | 8q23.1-q24.12 | 1 in 100,000 births |
| Angelman/Prader-Willi syndrome | Neurological and developmental disorders. | 15q11.2-q13.1 | 1 in 10,000–20,000 births |
Bring the Select Syndrome ScreenSM test
to your clinic
Check if the Select Syndrome Screen test is currently approved and available for use in your region.
Ready to Transform Your Genetic Screening?
For the Science Behind the Innovation
Discover how PTA and AI-driven analysis deliver new genetic insights.
The Profound Impact
Undetected microdeletions and microduplications may be associated with pregnancy loss, birth defects or developmental and intellectual disabilities.4,5
Our test is designed to detect these hidden risks early—before transfer—enabling proactive decision-making.


More informed embryo prioritization
Select Syndrome Screen isn’t just for high-risk cases—it’s for every patient undergoing PGT-A. It is designed to identify specific de novo (e.g., not inherited from either parent) microdeletion and microduplication syndromes that can affect anyone, of any age, going through IVF.7,8
When rare syndromes are detected before transfer, early education between patients and clinicians may provide better discussions on reproductive options and potential outcomes.

For Clinical Implementation
Learn how Select Syndrome Screen enhances patient care and streamlines your clinic’s genetic testing protocols.

For Patient Education
Access materials that help patients understand the benefits of enhanced genetic screening.

Ready to Get Started?
Connect with a CooperSurgical representative to discuss implementing Select Syndrome Screen in your clinic.
Frequently Asked Questions
Do you have questions about this new test? We have the answers. Find out how Select Syndrome Screen differs from standard PGT-A, and what the results mean for your patients.
Download the FAQ’s here.
What is Select Syndrome ScreenSM?
Select Syndrome Screen is an optional test that may be added to any of our PGT test offerings. It screens for genetic changes (microdeletions and microduplications) associated with the following syndromes:
- 1p36 deletion syndrome
- 2q33.1 deletion syndrome
- Angelman/Prader-Willi syndromes (15q11.2-q13.1)
- Cri-du-chat syndrome
- 22q11.2 deletion syndrome (DiGeorge / Velo-Cardio-Facial syndrome)
- Jacobsen syndrome
- Langer-Giedion syndrome
- Potocki-Lupski syndrome
- Smith-Magenis syndrome
- Wolf-Hirschhorn syndrome
Who is Select Syndrome Screen suitable for?
Select Syndrome Screen can provide valuable insights for any patient, regardless of their underlying risk profile. Select Syndrome Screen is meant for patients who do not have a known personal or family history of these syndromes. For patients with a known personal or family history of these disorders, PGT-M may be an option.
Does CooperSurgical recommend re-biopsy for a non-informative Select Syndrome Screen test result?
No. Non-informative results are most often due to inherent sample properties, such as reduced SNP density in that region. A re-biopsy is unlikely to change the outcome of testing.
What is the Genetic PN (Pronuclei) Check now included in our PGT-A test?
The Genetic PN Check identifies true 2PN embryos from morphologically reported 0, 1, and 3PN embryos. With the introduction of PTA, CooperSurgical is now able to perform PN checking without parental DNA, and CooperSurgical now offers this with PGT-A at no additional cost.
Please note that CooperSurgical does not report on uniparental disomy (UPD) or loss of heterozygosity (LoH) with PGT-A (Including Genetic PN Check).
How does the Genetic PN Check in our PGT-A (Including Genetic PN Check) test differ from our previous PGT-CompleteSM test?
The Genetic PN Check now included in our PGT-A test acts as a genetic fertilization check and ensures there are 2 copies of each chromosome present. Because CooperSurgical does not request cheek swabs in this test, it cannot confirm that equal amounts of DNA from both gamete providers are present. For a genetic PN check and biparental PN check, please advise your customer to order PGT-CompleteSM (parentage testing).
How does PGT-Complete (parentage testing) differ to our previous PGT-Complete test?
With the introduction of PTA, PGT-Complete (parentage testing) now has an increased accuracy of > 99.99% . The test still requires cheek swabs from both intended parents, and still includes all the features and benefits of the previous PGT-Complete test:
- Parentage confirmation* AND
- Origin of aneuploidy
- Bi-parental PN check*
*Not reported in countries where it is not permitted by regulatory bodies.
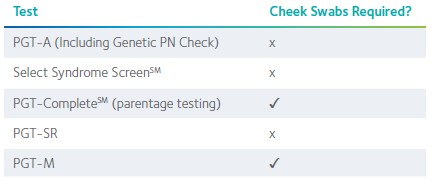
Which tests require parental cheek swabs from gamete contributors?
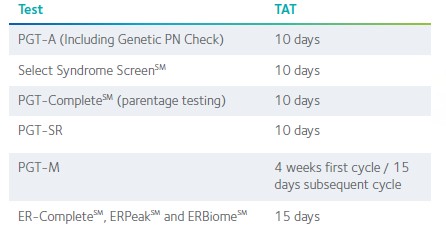
What are the turnaround times of our tests?
PGT-M ordering and reporting options
US version:
PGT-A testing is now included in all PGT-M cases but will be reported as per the preferred option selected on the new TRF. The default option on the new TRF is to report PGT-A on all embryos (previously Simultaneous PGT-A). Other options:
- Do not report PGT-A
- Retrospective PGT-CompleteSM (parentage testing)
- Please note that retrospective PGT-Complete (parentage testing) will be reported and billed for all embryos within that case.
INTERNATIONAL version:
PGT-A testing is now included in all PGT-M cases but will be reported as per the preferred option selected on the new TRF. The new default option is to report PGT-A on all embryos. Other options:
- Report PGT-A on unaffected/carrier embryos only
- Do not report PGT-A
Where can I get a copy of the new TRF?
You can download a copy of the new TRF from our resource page which includes a detailed overview of the TRF and report template updates: https://www.coopersurgical.com/coopersurgical-genomics-trf-and-report-updates/
From when must the new TRF be used?
Effective January 26th 2026, CooperSurgical will only accept the new global TRF.
Can Select Syndrome ScreenSM be ordered retrospectively?
No, due to laboratory processes, Select Syndrome Screen can only be ordered prospectively.
Can PGT-CompleteSM (parentage testing) be ordered retrospectively?
Yes, PGT-Complete (parentage testing) can be ordered retrospectively. Check with us prior to ordering that samples are eligible for retrospective PGT-Complete (parentage testing). Please note that PGT-Complete (parentage testing) will be reported and billed for all embryos within the case.
From when must the new PGT Patient Consent be used?
Effective January 15th 2026, CooperSurgical will only accept the new consent form.
How is Select Syndrome ScreenSM ordered?
Select Syndrome Screen can be ordered using the checkboxes on the new global TRF.
Select Syndrome Screen is available as an additional test option in addition to:
- PGT-A (Including Genetic PN Check) or
- PGT-SR or
- PGT-M (when receipt of PGT-A results is also selected)
- As well as with/without PGT Complete (parentage testing)
PGT-CompleteSM (parentage testing) is available as an additional test option in addition to:
- PGT-A (Including Genetic PN Check)
- PGT-SR or
- PGT-M (when receipt of PGT-A results is also selected)
- As well as with/without Select Syndrome Screen
Can I order Select Syndrome Screen and/or PGT-Complete (parentage testing) on a PGT-M or PGT-SR case?
Yes. Select Syndrome Screen and/or PGT-Complete (parentage testing) can be ordered using the checkboxes on the new global TRF under PGT-A, PGT-SR, or PGT-M (when receipt of PGT-A results is also selected).
I want to order PGT-M without PGT-A, or with PGT-A only on some embryos. How can I do that?
The new TRF simplifies our PGT-M options. PGT-A testing is now included in all PGT-M cases but will be reported as per the preferred option selected on the new TRF. The default option on the new global TRF is to report PGT-A on all embryos.
Do patients get genetic counseling with PGT Complete (parentage testing) or Select Syndrome Screen tests?
Recorded genetic counseling education will be available free of charge. Select Syndrome Screen genetic counseling will be available for a fee.
How is Select Syndrome Screen different from CooperSurgical’s standard PGT-A?
Select Syndrome Screen is a test specifically targeting regions where known syndromes occur due to recurrent, well documented deletions or duplications, which are often smaller and outside of the resolution of standard PGT-A.
Do patients still need prenatal testing for these syndromes?
Patients are recommended to speak to their clinician about what is available. It is important to note that Select Syndrome Screen is NOT a replacement for NIPT or diagnostic testing via chorionic villus sampling (CVS) or amniocentesis. Prenatal diagnosis is recommended for all pregnancies following PGT-A, with or without Select
Syndrome Screen.
Can Select Syndrome Screen be added to selected embryos?
Select Syndrome Screen is a prospective test only when added with PGT-A or PGT-SR. All biopsy samples for that patient case will be tested.
Can Select Syndrome Screen be added to PGT-M only?
No. However, you can opt for Select Syndrome Screen with PGT-M in conjunction with PGT-A or PGT-SR. Select Syndrome Screen will be tested on all PGT-A and PGT-SR samples for that patient case.
Can biopsied samples be sent as soon as a test order is submitted?
Yes. The Select Syndrome Screen test does not require parental DNA samples or an additional preparation period.
It follows the same streamlined workflow as PGT-A, allowing for immediate submission of biopsied embryo samples once the test order is placed. If ordering in addition to PGT-SR or PGT-M case review and assessment are still necessary before biopsies can be sent.
Are there cases that will not qualify for Select Syndrome Screen?
Select Syndrome Screen is meant for patients who do not have a personal or family history of one or more of these syndromes. For patients who do have a personal or family history of one or more of these syndromes, PGT-M may be suitable.
Will family members be required for test development?
No, family members are not required for Select Syndrome Screen as no test development is needed.
Can mosaicism be masked for PGT-A with Select Syndrome Screen?
Yes. The request to mask mosaicism for PGT-A can still be ordered in conjunction with Select Syndrome Screen.
Is there a potential for a mosaic result with Select Syndrome Screen?
Select Syndrome Screen will not report a mosaic result for the conditions tested by Select Syndrome Screen. Mosaic PGT-A results will still be reported.
Can PGT-CompleteSM be ordered with the Select Syndrome ScreenSM test?
Yes, but parent of origin is NOT reported for any sample with one of the designated microdeletions or microduplications. However, would be reported for a non-related aneuploidy in the PGT-A column.
If a sample receives a no result, will it apply to a specific syndrome on the panel or to the entire panel? How will this appear on the report from CooperSurgical?
If the PGT-A is a no result there will be a no result given for Select Syndrome Screen. For the Select Syndrome Screen each syndrome is reported individually.
What happens if a sample yields a non-informative result for a specific syndrome?
In rare cases where a sample does not yield a result, CooperSurgical does not recommend a re-biopsy.
How will non-informative results be reported?
The specific syndrome(s) not producing a result will be indicated in the Select Syndrome Screen report column.
Why would the test obtain a non-informative result?
It typically means that there were not enough informative SNPs (single nucleotide polymorphisms) in the region of interest to make a confident call. This is a technical limitation related to the data itself, not a reflection of biopsy quality or embryology technique. For microdeletion and microduplication testing, embryology-related factors are generally not a significant contributor to no result (NR) outcomes when the sample has otherwise produced a result for PGT-A.
Will CooperSurgical report other microdeletions or microduplications within the stated region for these particular syndromes?
No. This is a targeted test for known locations, and CooperSurgical reports within the test parameters. CooperSurgical will not report additional findings outside of the 10 syndromes included in the Select Syndrome Screen test.
If an embryo gets a positive result, does CooperSurgical offer re-biopsy to confirm?
No, re-biopsy is not offered to follow up on a positive microdeletion and microduplication result.
Can CooperSurgical discern whether a microdeletion or microduplication is meiotic vs mitotic?
No, our platform does not report whether a microdeletion or microduplication is meiotic or mitotic in origin.
Is Select Syndrome Screen compatible with both fresh and frozen cycles?
Our turnaround time for PGT-A is 10 days from sample receipt. CooperSurgical does not offer expedited testing for fresh transfers.
Are Select Syndrome Screen results stored or shared by CooperSurgical for future research or genetic database purposes?
Our research parameters are part of our patient consent.
Is this test covered by insurance?
Select Syndrome Screen is a proprietary test and is not currently covered by insurance.
Important Ordering, Consent And Reporting Updates
In preparation for the launch of the Select Syndrome Screen℠ test, we are updating the Test Requisition Form (TRF), consent and the report templates. To help you prepare, we’ve created a resource page with a detailed overview of the TRF and report template updates, including a presentation and video walkthrough.
Ready to Transform Your Genetic Screening?
For the Science Behind the Innovation
Discover how PTA and AI-driven analysis deliver unprecedented genetic insights.
Download the White Paper
References
- Weier, C. (2025) Select Syndrome ScreenSM White Paper. CooperSurgical, Inc. internal publication.
- Weier, C., et al. (2025) PGT-A incorporating sensitive and specific detection of nine recurrent microdeletion and microduplication syndromes using high resolution targeted sequencing [poster presentation]. PCRS Annual Conference, 2025
- American College of Obstetricians and Gynecologists, 2020. Preimplantation genetic testing: ACOG Committee opinion, Number 799. Obstetrics and Gynecology, 135.
- Wetzel, A.S., et al. (2022) A comprehensive list of human microdeletion and microduplication syndromes. BMC Genomic Data, 23(1), p.82.
- Maisenbacher, M.K. et al. (2023) Investigating the Incidence of the 22Q11.2 Deletion Syndrome in Miscarriage. ASRM Abstracts, Vol. 120, No. 4, Supplement, October 2023, e82.
- Watson, C.T., et al. (2015) The Genetics of Microdeletion and Microduplication Syndromes: An Update. Annu Rev Genomics Hum. 15; 215-244.
- McKinley Gardner, R.J., et al. (2018) Gardner and Sutherland’s Chromosome Abnormalities and Genetic Counselling. 5th ed. Oxford: Oxford University Press.
- Larroya, M., et al. (2021) Have maternal or paternal ages any impact on the prenatal incidence of genomic copy number variants associated with fetal structural anomalies? PLoS ONE, 16(7), p.e0253866.
Select Syndrome Screen is a genetic test intended only as a screening tool, which is designed to evaluate embryos for certain syndromes or chromosomal abnormalities. It is not a diagnostic test and cannot detect all genetic or health conditions. Healthcare providers should review the test’s indications, limitations, and potential risks and discuss these with their patients to determine whether the test is appropriate for the patient’s individual circumstances. Results for Select Syndrome Screen should be interpreted in the context of other clinical information and are subject to limitations such as mosaicism and technical variability. Medical guidelines and healthcare providers recommend that any pregnancy resulting from an embryo screened with this test undergo confirmatory diagnostic testing, such as chorionic villus sampling (CVS) or amniocentesis, to verify genetic status.