CooperSurgical has acquired ZyMōt Fertility, a subsidiary of DxNow, Inc. Read the full announcement here.

CooperSurgical ART Scientific Articles
-

ART Scientific Newsletter: The BIG FREEZE – Latest trends in oocyte vitrification
Introduction Human oocyte cryopreservation (OC) has gained immense popularity in the last decade. Post removal of the experimental label of…
-
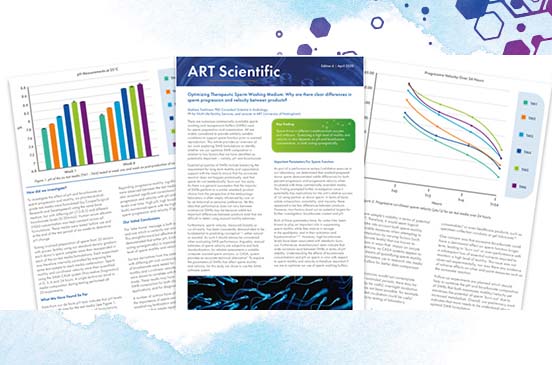
ART Scientific Newsletter: Optimizing Therapeutic Sperm Washing Medium
Optimizing Therapeutic Sperm Washing Medium: Why are there clear differences in sperm progression and velocity between products? There are numerous…
-
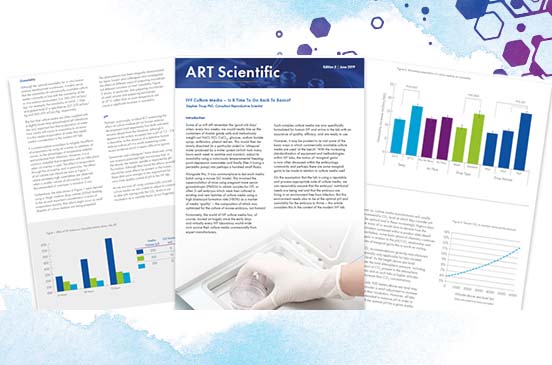
ART Scientific Newsletter: IVF Culture Media – Is It Time To Go Back To Basics?
Introduction Some of us will still remember the ‘good old days’ when, every two weeks, we would neatly line up…
-
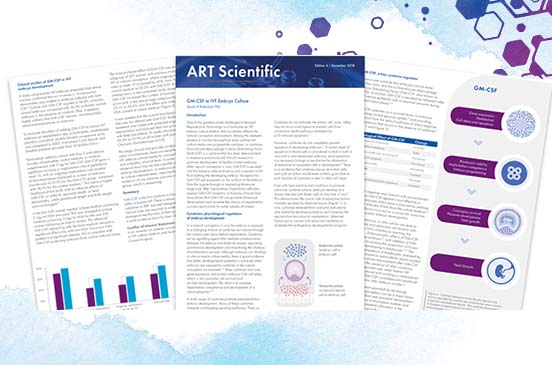
ART Scientific Newsletter: GM-CSF in IVF Embryo Culture – An Update
Introduction An ongoing challenge in ART culture media formulation is to provide the survival factors that support embryos through the…
-
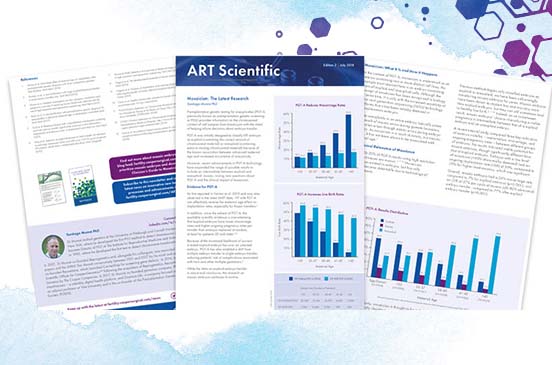
ART Scientific Newsletter: Mosaicism: The Latest Research
Preimplantation genetic testing for aneuploidies (PGT-A, previously known as preimplantation genetic screening or PGS) provides information on the chromosomal content…
-
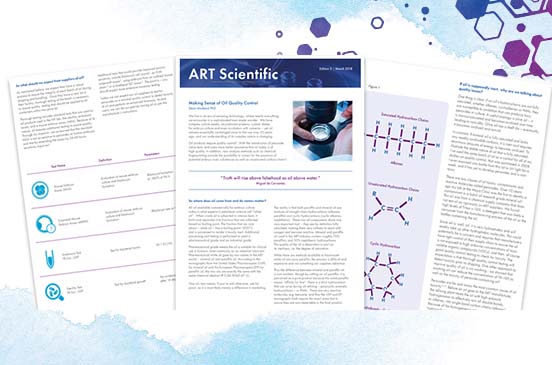
ART Scientific Newsletter: Making Sense of Oil Quality Control
We live in an era of amazing technology, where nearly everything we encounter is a sophisticated man-made wonder. We have…
-
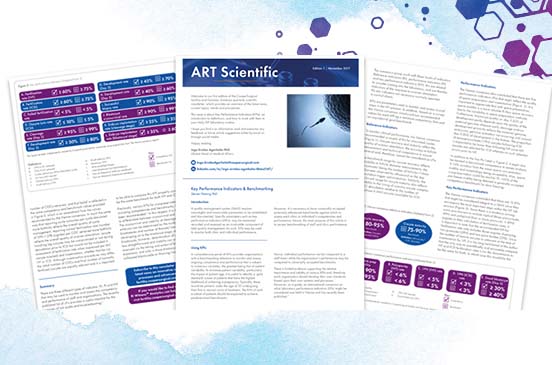
ART Scientific Newsletter: Key Performance Indicators & Benchmarking
Introduction A quality management system (QMS) requires meaningful and measurable parameters to be established and documented. Specific parameters such as…
-
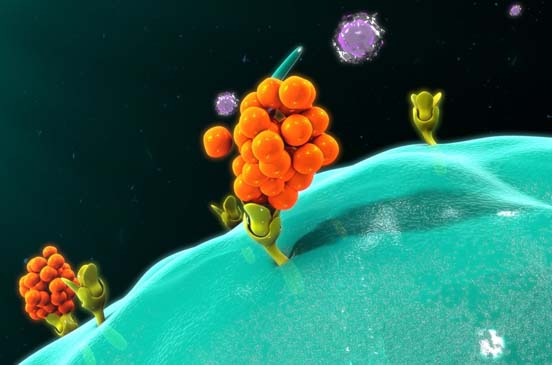
Why are we adding the GM-CSF Cytokine to our Culture Media?
EmbryoGen® and BlastGen™ were the first sequential media commercially available to contain the cytokine, Granulocyte-Macrophage Colony-Stimulating Factor (GM-CSF). In this article,…

Get In Touch With Us
We’d love to hear from you. How can we help?